A guide for new fathers — and a reframe of postpartum support around an underserved point of intervention: the father, not the mother.
Postpartum care conventionally treats the mother as the primary — often sole — subject of support. This project starts from a different premise: the father, as the mother's support system, is a more durable and far less designed-for point of intervention. Strengthening that role strengthens the whole household, not just one person in it. It's the insight everything else in this project follows from.
Postpartum (or postnatal) depression is a mood disorder associated with childbirth — clinically, a non-psychotic depressive episode diagnosed under "depressive disorder with peripartum onset," where onset falls anytime during pregnancy or within four weeks of delivery. It can affect anyone who has given birth or adopted, including women with a history of miscarriage, bipolar disorder, or a family history of the condition, regardless of sexual orientation.
Left unaddressed, it can become chronic. It affects an infant's growth, behavior, and bonding with the mother; strains the mother's relationships with her spouse and family; and in its most severe form, can lead to psychosis, self-harm, or harm to the infant.
These figures come from secondary research at the time of the original project (WHO and contemporaneous clinical sources), cited here as they informed the original design decisions.
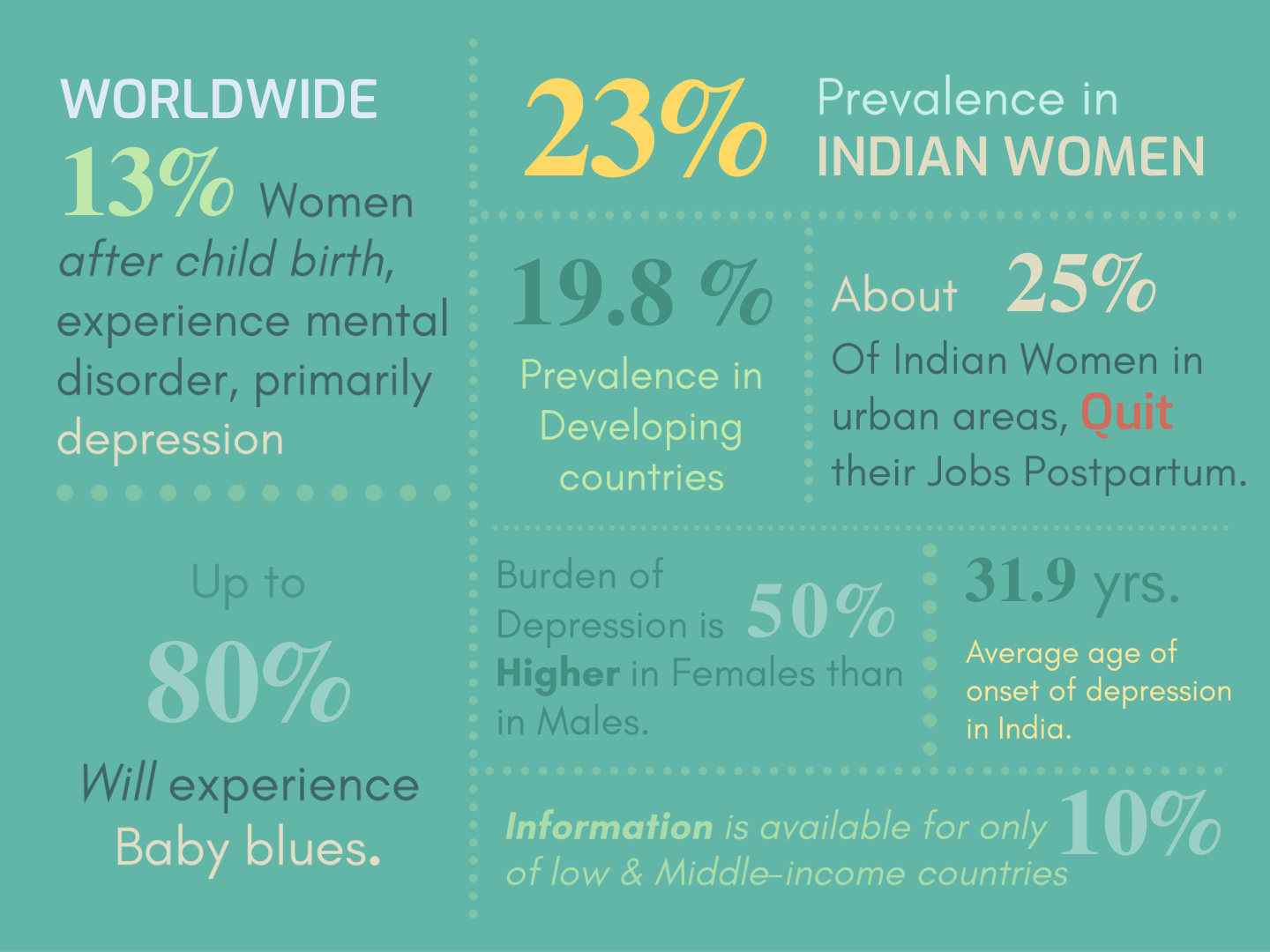
Sources: Mapping global prevalence of depression among postpartum women, Translational Psychiatry · Prevalence of postpartum depression at subnational level in India, Women & Health · Prevalence of Post-Partum Depression in India, National Journal of Community Medicine
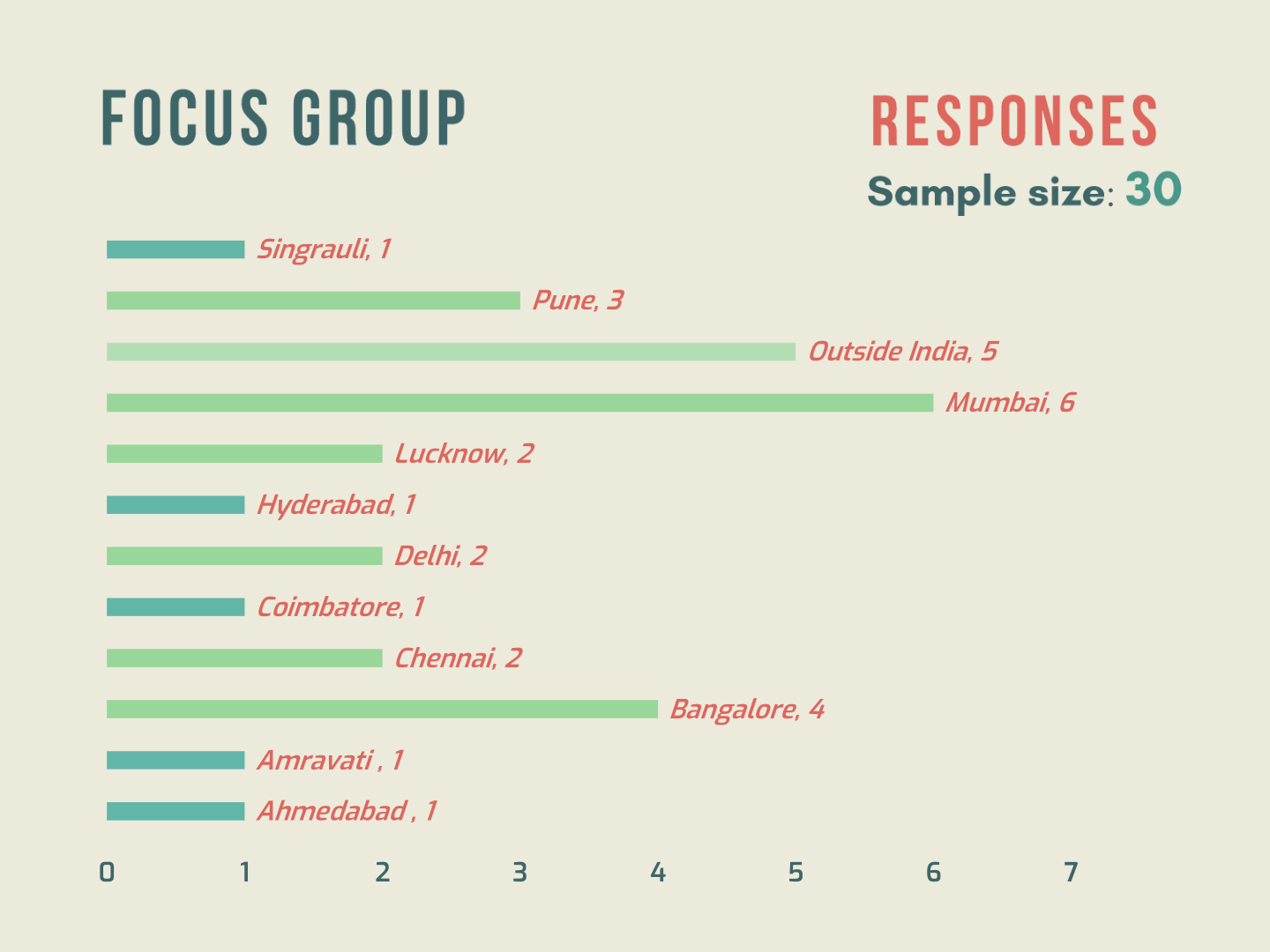
The focus group centered on Indian, urban, first-time mothers aged 26–35, currently or previously working. An "un-focus" group of new fathers, gynecologists, obstetricians, psychiatrists, and peers of the same age range provided a second lens on the same problem. The survey drew 30 respondents across Indian cities — Mumbai, Bangalore, Pune, Delhi, Chennai, and others — plus a small group based outside India.

Mapping who actually surrounds a new mother — spouse, family, friends, medical providers, colleagues — made it clear that care for her is distributed across a wide, uneven network. Some of that network needs to be informed, some needs to recognize and treat, some just needs to be sensitized. But one relationship sits closer and more constantly than any other: the spouse.
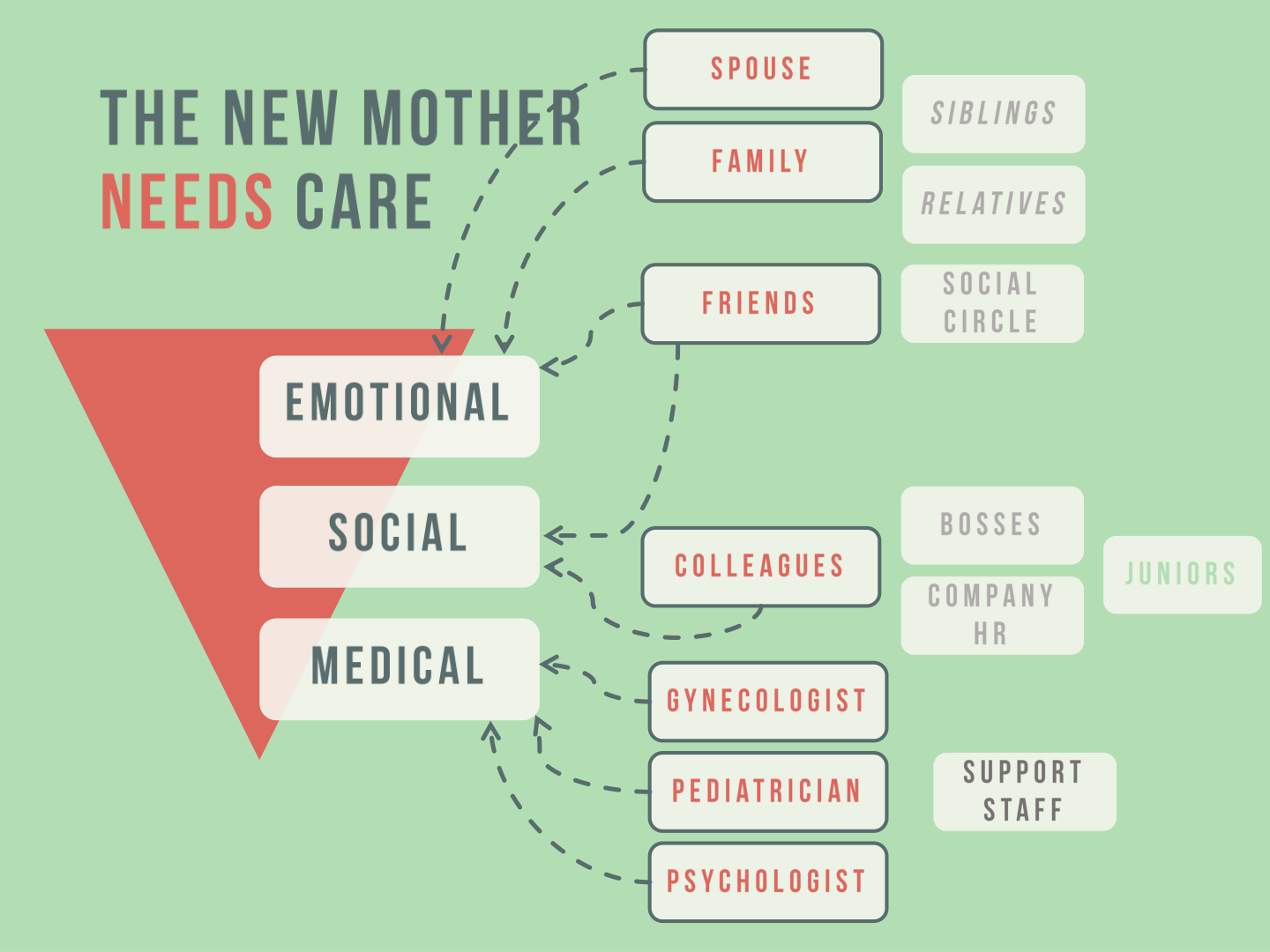
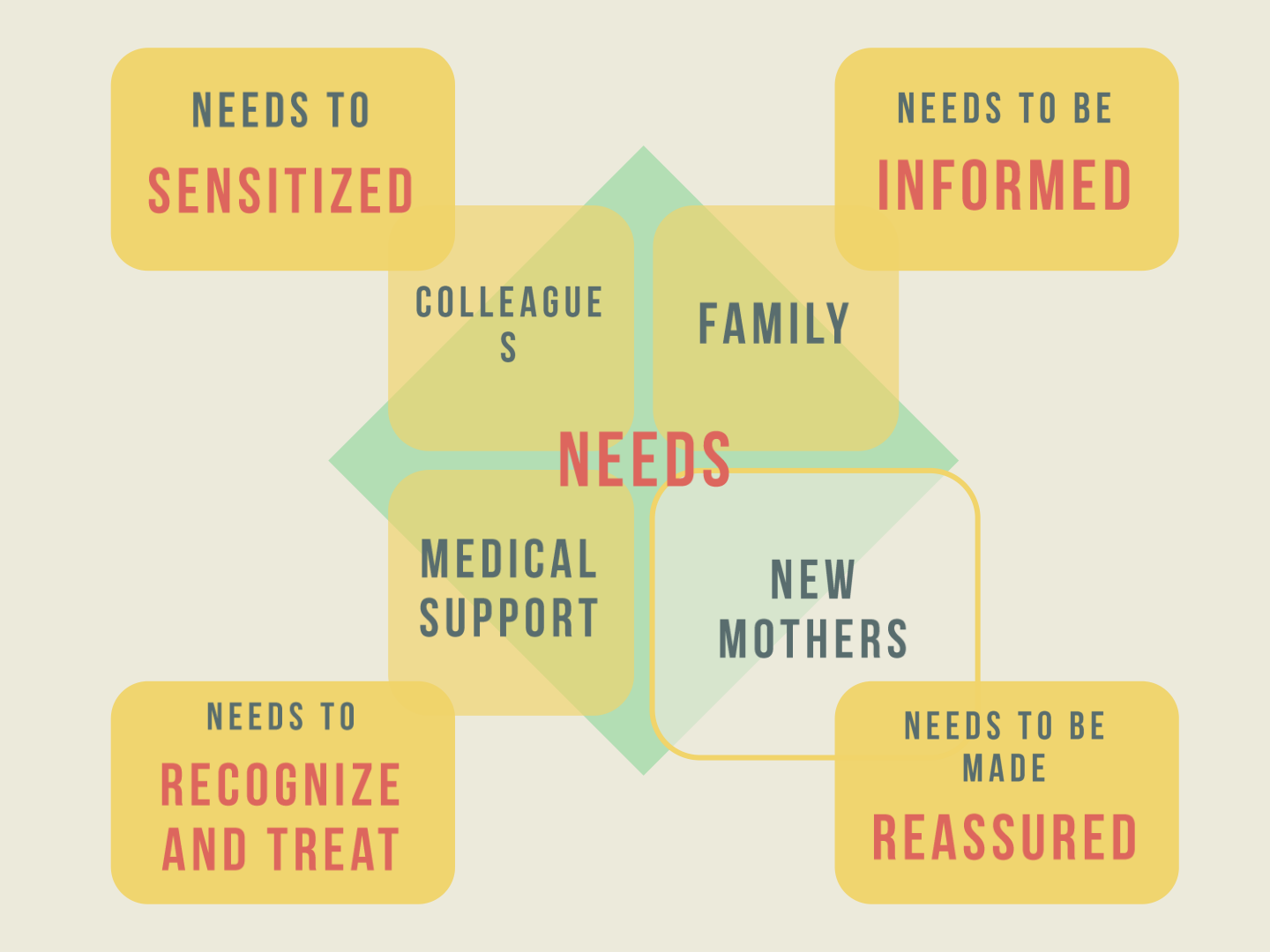
Everyone in that network has a role. But the father is the one person positioned to act every day, in the home, without needing a medical referral or a scheduled visit — which made him the highest-leverage, least-designed-for point of intervention.
Early explorations leaned toward poster-style illustration — dense line work aimed at telling a fuller story. Jury feedback in the first review was direct: the drawings read more like novel illustrations than something a reader could absorb in the few seconds a poster allows. That pushed the direction toward something simpler and faster to read, which is what ultimately shaped the manual format — short, illustrated, one instruction per spread.
The result was The Side-kick's Manual — a short, illustrated guide addressed directly to new fathers, opening with a plain explanation of what postpartum depression is and isn't, followed by five concrete actions.
The reframe is the part of this project worth leading with, more than the process that got there. It would have been easy to build another resource aimed at the mother — the research field is full of them. Redirecting the intervention toward the person already closest to her, already in the house, already capable of acting without a system's permission, is the idea that still holds up years later, including against the updated numbers above.
This case study draws on the original 2017 NID thesis document, research, and interviews. If you'd like more of the process work — early poster explorations, jury feedback rounds, or the full interview notes — I can add them here.